
Abdalla Daloul
Biomedical Engineering Undergraduate Senior, Imaging concentration
Email:
Week 1: Good Design and Bad Design Heading link
We had the incredible opportunity to meet with Dr. Young, director of urology innovation and technology, as well as the director of the Urology Lab at the UIC Innovation Center. We were introduced to the rest of the professionals in the Urology department. Our first day started with a visit to the operating room, where we witnessed a surgery involving the removal of a kidney tumor. On the third day at the operating room, we observed Dr. Garvey performing five back-to-back procedures such as cystourethroscopy injections, biopsies of scrotal lesions and co2 laser, cystourethroscopy biopsy, ureteroscopy and cystourethroscopy TURBT. As the week progressed, we transitioned to the clinic setting, where we excitedly observed various procedures, including cystoscopy and vasectomy.
Good Design: Surgeon console of the da Vinci surgical system
The surgeon console of the da Vinci surgical system, which is part of the endoscopic instrument control system, is highly regarded as a well-designed tool. It is commonly used in urology because it offers precise control, better visibility, and minimally invasive procedures. The console’s ergonomic design keeps surgeons comfortable during surgeries, and its advanced technology helps improve surgical capabilities. Urologists prefer using this system because it has shown positive results in clinical outcomes. Overall, it helps urologists provide better care and achieve successful outcomes for their patients. I was really impressed by the da Vinci surgical system; it looked like a video game come to life, and I was completely fascinated by what it could do. Dr. Crivellaro, who was incredibly skilled, finished the procedure and then asked one of the doctors to suture the kidney. He kindly sat next to her, providing assistance and guidance throughout the process.
Looking at this design through the AEIOU framework to the endoscopic instrument control system, such as the surgeon console of the da Vinci surgical system:
Activities: Doctors would be performing surgical procedures using the endoscopic instrument control system. This involves manipulating the surgical instruments and controlling their movements through the surgeon console.
Environment: The environment includes the operating room where the surgical procedures take place, and the placement as well as the setup of the da Vinci system. Factors such as lighting, ergonomics, and the organization of equipment would be considered.
Interactions: Doctors would interact with the team, including assisting nurses and other doctors. They would also communicate with the patient before the procedure. Interactions with the da Vinci system would involve hand-eye coordination and precise control of the instruments.
Objects: Would be the surgical instruments and tools used with the da Vinci system, as well as the components of the surgeon console itself, such as the master controls, foot pedals, and display.
User: Doctor overall user experience would involve their subjective impressions, including their comfort level, proficiency with the system, and perceptions of the system’s effectiveness and efficiency in assisting their surgical tasks.
Bad Design: Wires lying around in the operating room
Having wires lying around in the operating room can be a big problem for nurses and doctors. It can be dangerous and cause accidents or injuries. The messiness and disorder created by scattered wires can make it hard for healthcare providers to move around and work efficiently during surgeries. It can also lead to contamination and make it difficult to maintain cleanliness and prevent infections. Using tape to control the wires is not a good idea because it might not keep them organized, and the sticky residue can make things even worse. It’s important to have a better system for managing the wires to ensure a safe and organized operating room.
Looking at this design through the AEIOU framework:
Activities: Using tape to control wires aims to organize them, but it may not work well because the tape may not hold the wires securely.
Environment: Loose wires in the operating room can be unsafe. If tape is used to control them, it may not be effective, increasing the risk of tripping or accidentally disconnecting medical equipment.
Interactions: Tape can interfere with interactions among healthcare providers as it can make it difficult to find and access wires and equipment quickly. This can affect communication and collaboration during surgeries.
Objects: Tape is a concern in this case. It may seem like a quick solution, but it’s not a good design choice as it may not reliably manage the wires.
Users: Nurses, doctors, and other healthcare providers are directly affected by using tape to control wires. It can cause challenges and disruptions for them.
Overall using a tape as a solution to control wires in the operating room can be considered a bad design because it may not effectively manage the wires, leading to disorganization, safety hazards, and potential disruption of surgical procedures. Implementing more robust wire management systems, such as cable management solutions, is necessary to ensure a safe, organized, and efficient operating room environment.
Week 2: The Storyboard of Shock Wave Lithotripsy Heading link
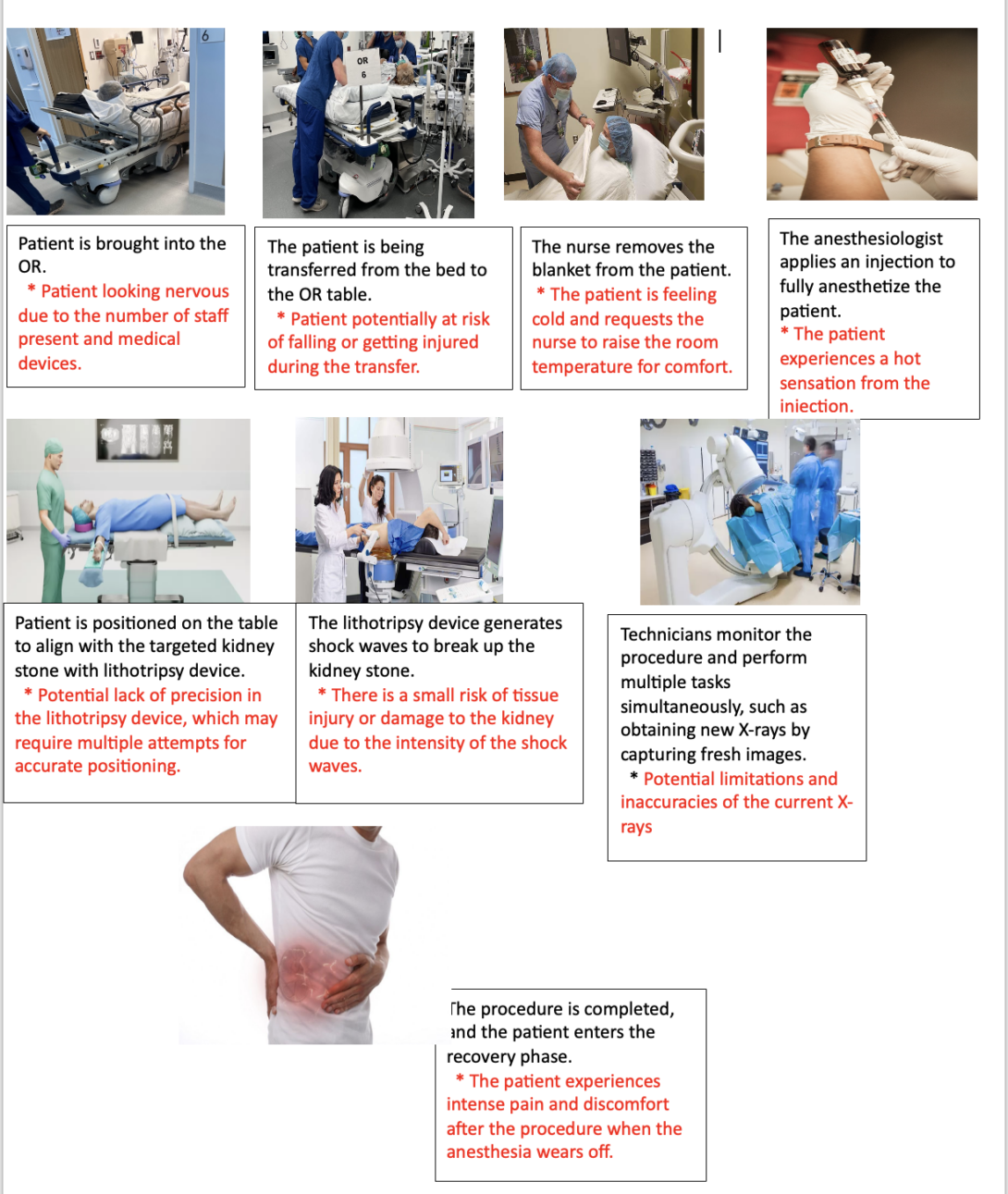
Kidney stones are hard deposits that form in the kidneys. They are typically composed of minerals and salts that crystallize and accumulate over time. Kidney stones can vary in size and may cause severe pain and discomfort when they block the urinary tract. Traditionally, open surgery was commonly employed to remove these stones, but it carried inherent challenges and risks. However, the introduction of shock wave lithotripsy (SWL) revolutionized the treatment of urinary stones by offering a noninvasive alternative.
Shock wave lithotripsy is a noninvasive surgical technique used to remove urinary stones.
I found a research paper discusses about the advancements, limitations, and potential adverse effects of shock wave lithotripsy in the treatment of urinary stones. Before the introduction of SWL, open surgery was commonly used, which posed challenges and potential complications. SWL provided a noninvasive alternative by utilizing high-intensity acoustic pulses to break up urinary stones.
Sources for the images:
- April 29, 2021 – eNews Briefs. (n.d.). Outpatient Surgery Magazine. Retrieved July 17, 2023, from https://www.aorn.org/outpatient-surgery/article/2021-04-28-April-29-2021
- Extracorporeal Shockwave Lithotripsy – +371 67201005; ARS Diagnostic. (n.d.). Medicīnas Centrs ARS. https://arsmed.lv/en/ars-diagnostikas-klinika/lithotripsy/
- Hangee-Bauer, S. F. N. M. D. C. (2016, November 9). Hot Shots—The Latest Injection Therapies at SFNM. San Francisco Natural Medicine. https://www.sanfrancisconaturalmedicine.com/natural-health-news//latest-injection-therapies
- Lithotripsy for Large Kidney Stones: What to Expect: Urological Associates: Urologists. (n.d.). Www.cvilleurology.com. Retrieved July 17, 2023, from https://www.cvilleurology.com/blog/lithotripsy-for-large-kidney-stones-what-to-expect
- Patient positioning in the operating room · Incision. (2022, April 28). Incision. https://www.incision.care/blog/patient-positioning-in-the-operating-room
- Shockwave Medical | Cardiovascular Business. (n.d.). Cardiovascularbusiness.com. Retrieved July 17, 2023, from https://cardiovascularbusiness.com/sponsored/5020/shockwave-medical
- Tandan, M. (2011). Extracorporeal shock wave lithotripsy for pancreatic and large common bile duct stones. World Journal of Gastroenterology, 17(39), 4365. https://doi.org/10.3748/wjg.v17.i39.4365
Bailey, M., Maxwell, A. D., Cao, S., Ramesh, S., Liu, Z., Williams, J. C., Thiel, J., Dunmire, B., Colonius, T., Kuznetsova, E., Kreider, W., Sorensen, M., Lingeman, J. E., & Sapozhnikov, O. A. (2022). Improving Burst Wave Lithotripsy Effectiveness for Small Stones and Fragments by Increasing Frequency: Theoretical Modeling and Ex Vivo Study. 36(7), 996–1003. https://doi.org/10.1089/end.2021.0714
Week 3: Forming a Needs Statement Heading link
This week, primarily focused on observing OR procedures using DaVinci surgical robot. Also, focused on forming needs statements from which the scope of my observation in OR. There are three iterations of a need statement relating to technical issues with surgical displays during robotic surgeries.
First Iteration:
Medical staff face a critical problem as the surgical displays connected to the da Vinci robotic system experience persistent malfunctions and flickering, significantly impeding surgeries safety and efficiency.
Population: Medical staff
Opportunity: experience persistent malfunctions and flickering.
Outcome: impeding surgeries’ safety and efficiency.
Second Iteration:
Medical staff face a critical problem as the surgical displays connected to the da Vinci robotic system experience persistent malfunctions and flickering, having a severe impact on the safety and efficiency of surgeries.
Population: Medical staff.
Opportunity: Experience persistent malfunctions and flickering.
Outcome: Having a severe impact on the safety and efficiency of surgeries.
Reason: Replacing significantly impeding surgeries safety and efficiency with having a severe impact on the safety and efficiency of surgeries. Its more concise and straightforward while conveying the same idea. Also, it provides a clear and direct description of the problem consequences.
Third Iteration:
Medical staff continue to face a critical problem as the surgical displays connected to the da Vinci robotic system experience persistent malfunctions and flickering, having a severe impact on the safety and efficiency of surgeries.
Population: Medical staff
Opportunity: Experience persistent malfunctions and flickering.
Outcome: Having a severe impact on the safety and efficiency of surgeries.
Reason: added Continue to face, this change suggests that the problem has persisted over time and hasn’t been resolved yet. It emphasizes the urgency of finding a solution as the issue is ongoing and affecting medical staff’s ability to perform surgeries effectively.
source:
Tscholl, D. W., Handschin, L., Rössler, J., Weiss, M., Spahn, D. R., & Nöthiger, C. B. (2019). It’s not you, it’s the design – common problems with patient monitoring reported by anesthesiologists: a mixed qualitative and quantitative study. BMC Anesthesiology, 19(1). https://doi.org/10.1186/s12871-019-0757-z
Week 4: Patent Research Heading link
Needs statement: A device to reduce the presence of fine particles within surgical environments, particularly when surgical smoke-producing instruments are utilized by surgeons during procedures in operating rooms.
Patent: US10898622B2, Surgical evacuation system with a communication circuit for communication between a filter and a smoke evacuation device. The main claims of this patent is a filter device in communication with the smoke evacuation device through the communication circuit, wherein the filter device comprises a plurality of filter components. Additional claims, the communication circuit determines authenticity of the plurality of filter components by using filter component information. Also, recording by the communication circuit, errors output from the plurality of filter components.
Source: IV, F. E. S., Yates, D. C., Danziger, B. J., Harris, J. L., & Aldridge, J. L. (n.d.). Surgical evacuation system with a communication circuit for communication between a filter and a smoke evacuation device. Retrieved August 6, 2023, from https://patents.google.com/patent/US10898622B2/en?q=(surgical+smoke+system)&oq=surgical+smoke+system&page=2
Week 5: Total Addressable Market Calculation Heading link
Needs Statement:
A solution to decrease the concentration of fine particles in operating rooms is needed when tools that generate surgical smoke (electrosurgical tools and lasers) are being used by surgeons in operating rooms.
Population: Medical professionals preforming and assisting in the operating rooms
Opportunity: Electrosurgical tools are being used in surgery
Outcome: Decreased the risk of inhaling surgical smoke
Surgical smoke is the hazardous, generated during various surgical procedures that involve the use of surgical instruments such as lasers and electrocautery devices. The smoke can negatively impact the health and safety of medical staff, including surgeons, nurses, anesthesiologists, and other medical professionals present in the operating room. To address these concerns, surgical smoke evacuation systems, it’s designed to effectively capture and remove surgical smoke from the operating room environment. Based on my research, I found that electrosurgery is used in more than 85% of 24 million surgeries performed annually in the US, which is 20,400,00 million surgeries used electrosurgery. According to medical price online the total cost of the surgical smoke evacuation system is $3,150. o calculates the TAM I used the formula TAM = # of units/year * cost of product = 20,400,000 * 3,150 = 64,260,000,000. Total Addressable Market (TAM) is $64,26 Billion.
sources:
Average Surgical Smoke Evacuation System Price Quotes and Cost Information. (n.d.). Medical Price Online. Retrieved August 9, 2023, from https://www.medicalpriceonline.com/medical-equipment/surgical-smoke-evacuation-system/
Surgical Smoke Evacuation: a Survey of OR Nursing Staff. (2018, November 8). Smoke Free or – Stryker. https://www.smokefreeoperatingroom.com/surgical-smoke-evacuation-a-survey-of-or-nursing-staff/