
Rhys Gogonis
2024 students
Email:
Good Design vs Bad Design
Good Design
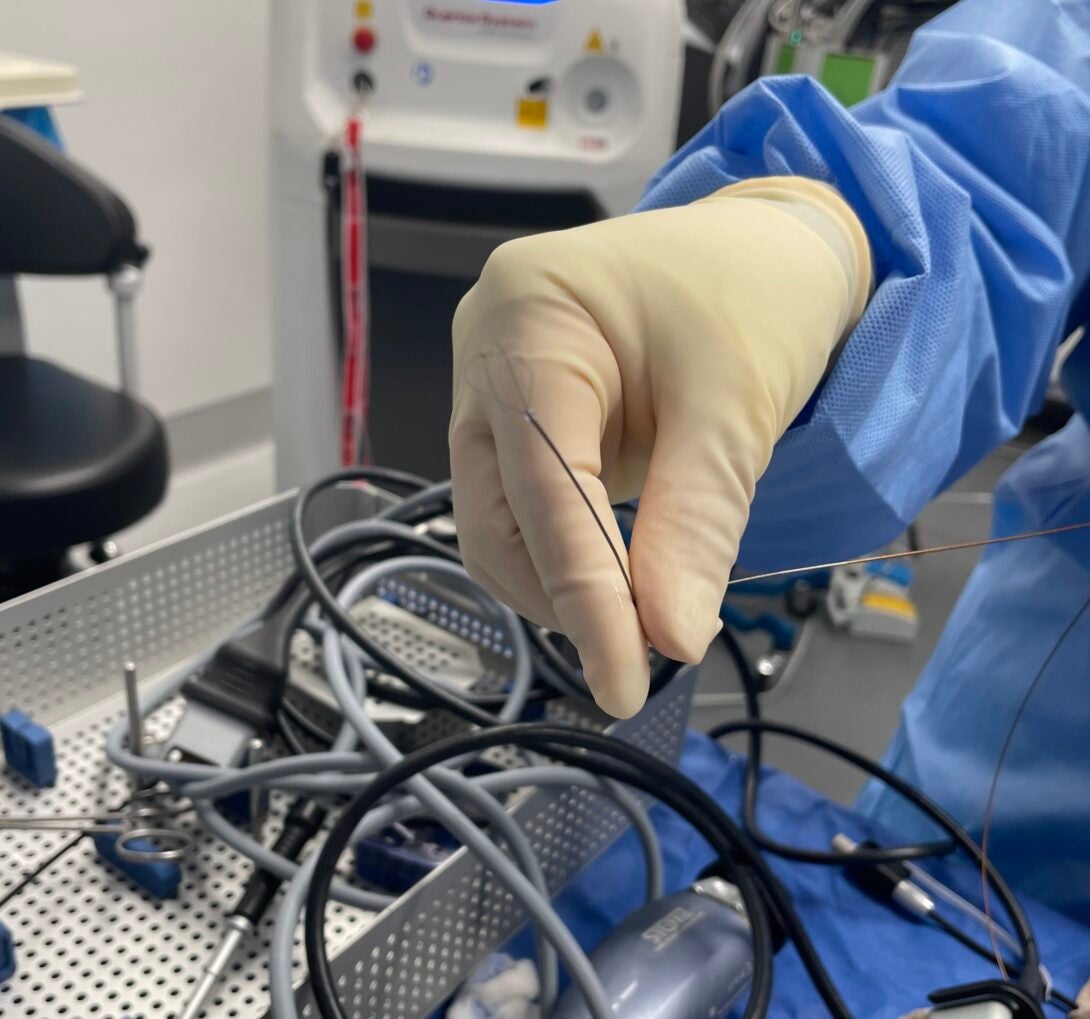
On Friday, June 28 I observed a kidney stone removal in the operating room. The kidney stone had advanced into a minor calyx of the right kidney. The stone was suspected to have advanced proximally from the mid ureter into the renal pelvis due to the ureter-cystoscope placement. In order for the surgeons to remove the stone, they must identify the stone, stabilize it, and blast it with a laser. To stabilize the stone, they use a very intriguing tool that advances through the sheath of the scope all the way to the calyxes. The tool, pictured below, is simply an arrangement of wire that looks similar to an egg-beater. The surgeon uses the wire to grasp the stone. The wire sort of balloons from the scope outward and once the stone is surrounded by wire, the surgeon can pull on the wire to secure the stone. Think of cookie dough becoming trapped within the wire loops of an egg beater. This prevents the laser from accidentally damaging the mucosa of the kidney. I believe this to be a simple yet elegant design to secure a stone in the kidney. The wire design minimally damages the mucosa (it’s simply a wire expanding) instead of clamps that might accidentally chomp down or pinch the kidney mucosa. There really isn’t many moving parts in this design, either, which minimizes error. The interaction between the surgeon and the tool is quite easy & minimal; the surgeon simply advances the wire so that the wires balloon outward. While there may be other designs that could be better, this is a beautiful design that accounts for cost, efficiency, ease-of-use, and effectiveness.
Poor Design
On Wednesday, June 26 I observed an out-patient (non-OR) stent removal procedure. The procedure is done with a disposable cystoscope. The cystoscope contains inflow & outflow tracts which allow for the surgeon to insert clamps or other tools. In this specific procedure, the surgeon inserts a clamp in order to grasp onto the stent and subsequently pull the stent through the urethra. One problem with this design is that the cystoscope and clamp requires two individuals to operate. One individual, the surgeon, is holding the cystoscope with their right hand and the penis or vagina with their left. The other individual is inserting & manipulating the clamp device in which they insert into a cystoscope port. I observed in clinic a lot of back and forth communication between the surgeon and the second operator. Much of the conversation included: “is the clamp open? Do you feel the stent within the clamp’s jaws? Advance the clamp”. That communication resulted in procedure delay, patient pain, and overall inefficiency. The extra communication also introduced many opportunities for procedure complications. I kept asking myself: why can’t one surgeon perform all of the dependent tasks themself? Why does this one tool require two operators? For these reasons and more, I believe this design could be improved to greatly reduce patient harm and procedure complications as well as improve timeliness.
Secondary Research & Patent Exploration

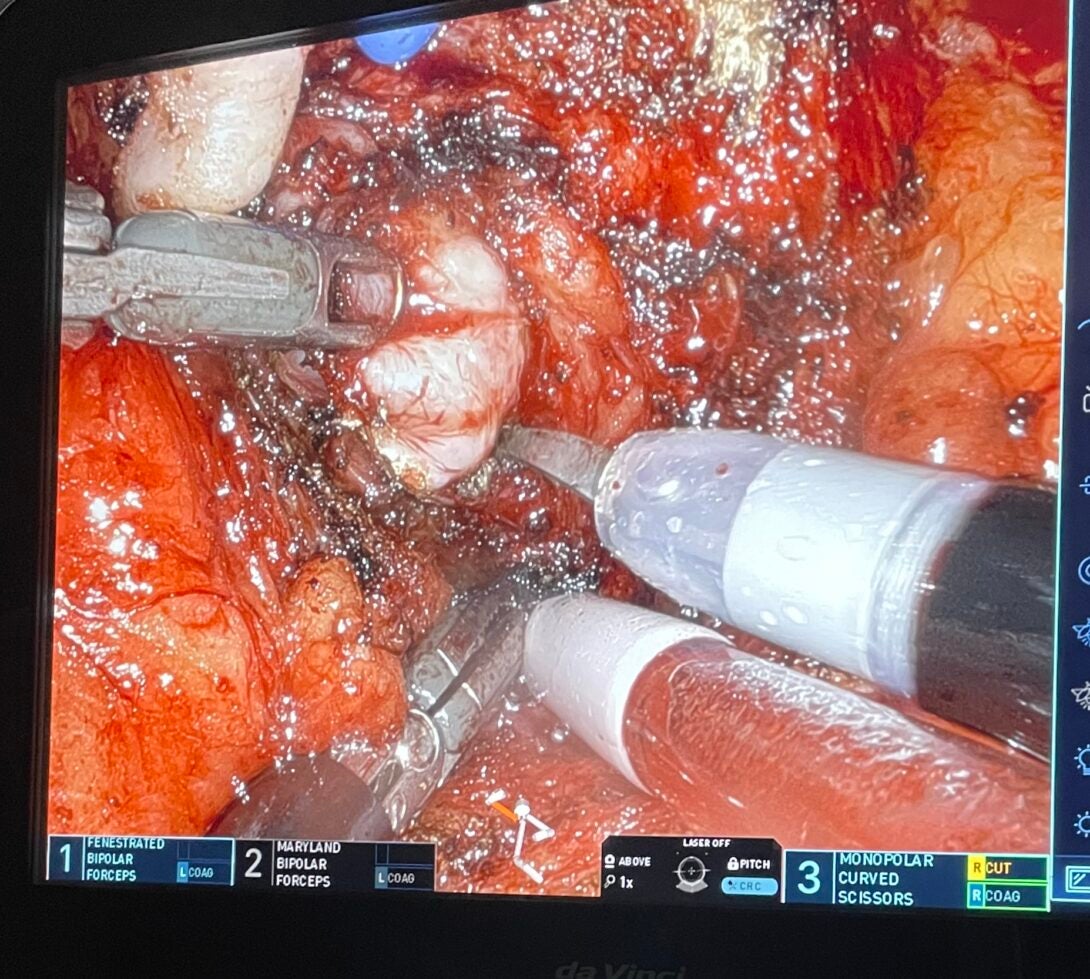
An interesting problem that we discovered during robotic-assisted prostatectomy related to ventilation & blood suction management. I wanted to look more into this issue and stumbled upon a research article in the journal of Endourology related to this idea.
The article “Impact of Surgeon-Controlled Suction During Robotic Prostatectomy to Reduce Dependence on Bedside Assistance” explores the implementation and effects of giving surgeons direct control over suction devices during robotic-assisted prostatectomies. Traditionally, the role of managing suction has been performed by a bedside assistant, but this study investigates whether surgeon-controlled suction can improve surgical efficiency and outcomes.
The researchers implemented a system where the surgeon, operating the robotic console, could control suction devices without needing assistance. This modification aimed to streamline the procedure, potentially reducing operation time, increasing precision, and minimizing interruptions. The study measured various parameters, including operative time, the frequency of needing bedside assistance, and intraoperative complications.
Findings indicated that surgeon-controlled suction significantly reduced dependence on bedside assistants. This led to a decrease in operative time and interruptions, contributing to a more seamless and efficient surgical process. Additionally, there was no increase in intraoperative complications, suggesting that surgeon-controlled suction is safe and effective.
Overall, the study concluded that empowering surgeons with direct control over suction during robotic prostatectomies can enhance procedural efficiency and reduce reliance on additional surgical personnel, potentially transforming standard practices in robotic surgery.
I also identified a patent on the device mentioned in this article, the “Remotely Operated Suction Irrigation” device (ROSI). The patent “Remotely Controlled Suction/Irrigation for Surgery” (US10561429B2) presents a system designed to enhance surgical procedures by allowing surgeons to control suction and irrigation devices remotely. This system aims to improve efficiency and precision during surgeries, particularly in minimally invasive and robotic-assisted procedures as we commonly see in CIP.
The system includes a remote control interface that can be integrated with the surgeon’s console in robotic surgeries. This interface allows the surgeon to manage suction and irrigation functions without relying on a bedside assistant. It is also designed to be modular, making it adaptable to various surgical setups and easy to integrate with existing surgical robots and tools. ROSI precise control over suction and irrigation parameters, such as flow rate and pressure, enhancing the surgeon’s ability to manage the surgical field effectively. Options for controlling the system include a foot pedal or a handheld controller, providing flexibility based on the surgeon’s preference and the specific requirements of the procedure. Built-in safety mechanisms ensure that the system operates within safe parameters, preventing potential harm to the patient due to excessive suction or irrigation.
Some advantages of ROSI include increased efficiency, precision, and ergonomics. By enabling surgeons to control suction and irrigation directly, the system reduces the need for constant communication and coordination with a bedside assistant, streamlining the surgical process. The precise control afforded by the system allows for better management of the surgical site, potentially leading to improved outcomes and reduced intraoperative complications. The ergonomic design of the control interfaces minimizes physical strain on the surgeon, contributing to better performance and reduced fatigue during long procedures.
Need statements
In my last blog post, I talked about blood suction devices used in tandem with single-port robotic surgery systems. Pulling from that, I developed a needs statement:
Surgeons using single-port Da Vinci robot system struggle with suction device control & manipulation during prostatectomy and need better suction control to reduce blood loss, reduce surgery down time, and reduce surgery preparation time.
My first needs statement was informed by observing robotic-assisted prostatectomies. During these surgeries, I observed a silk string tied to the end of the suction tube device. The purpose of this was to improve manipulation and control of the suction tubing tip. I found this very interesting. I asked further questions about the string tie method and I received comments such as “it is annoying but it’s the easiest way” and “I wish we had another [robotic] arm for suction, but it would limit us”. Currently in a single-port Da Vinci robot surgery, only 4 surgical arms are allowed in the surgical field at a time. So, using one of those arms for suction limits the surgeon’s ability for other maneuvers. In the POO format:
Population: Urologists performing prostatectomies
Opportunity: Vacuum tip control
Outcome: Improved surgical downtime
Total Addressable Market (TAM): $270 million
Serviceable Addressable Market (SAM): $80 million
Average surgical suction tubing: $140
# of Da Vinci robotic procedures (2022): 1,875,000
# of robotic SP prostatectomies: 72k
# of SP robotic hysterectomies: 480k
Needs statement: Urologists have difficulty with blood vacuum tip control during prostatectomy and need better suction control to improve surgical downtime.
Improved Needs Statement
This blog will cover my improved needs statement. I realized that I needed to be much more specific when describing the surgical context. I specified the population to limit this statement to urologists performing single-port robotic-assisted prostatectomies and hysterectomies, since these surgeries are similar. I also expanded the opportunity to talk more about the control and manipulation of suction as a whole during surgery. As far as the outcome, I completely changed these so that I included tangible metrics that can be measurable and are reliable.
Population: Urologists performing single-port robot-assisted surgery
Opportunity: Suction manipulation and control
Outcome: Reduced surgery downtime, preparation time and blood loss.
Improved Needs Statement: Surgeons using single-port Da Vinci robot system struggle with suction device control & manipulation during prostatectomy and need better suction control to reduce blood loss, reduce surgery down time, and reduce surgery preparation time